If you’ve looked at your 2026 Marketplace health insurance options and you’re feeling sticker shock because you’re seeing significantly larger premiums, don’t panic just yet. Here’s what you need to know as open enrollment for 2026 health coverage gets underway.
Who’s experiencing Marketplace sticker shock?
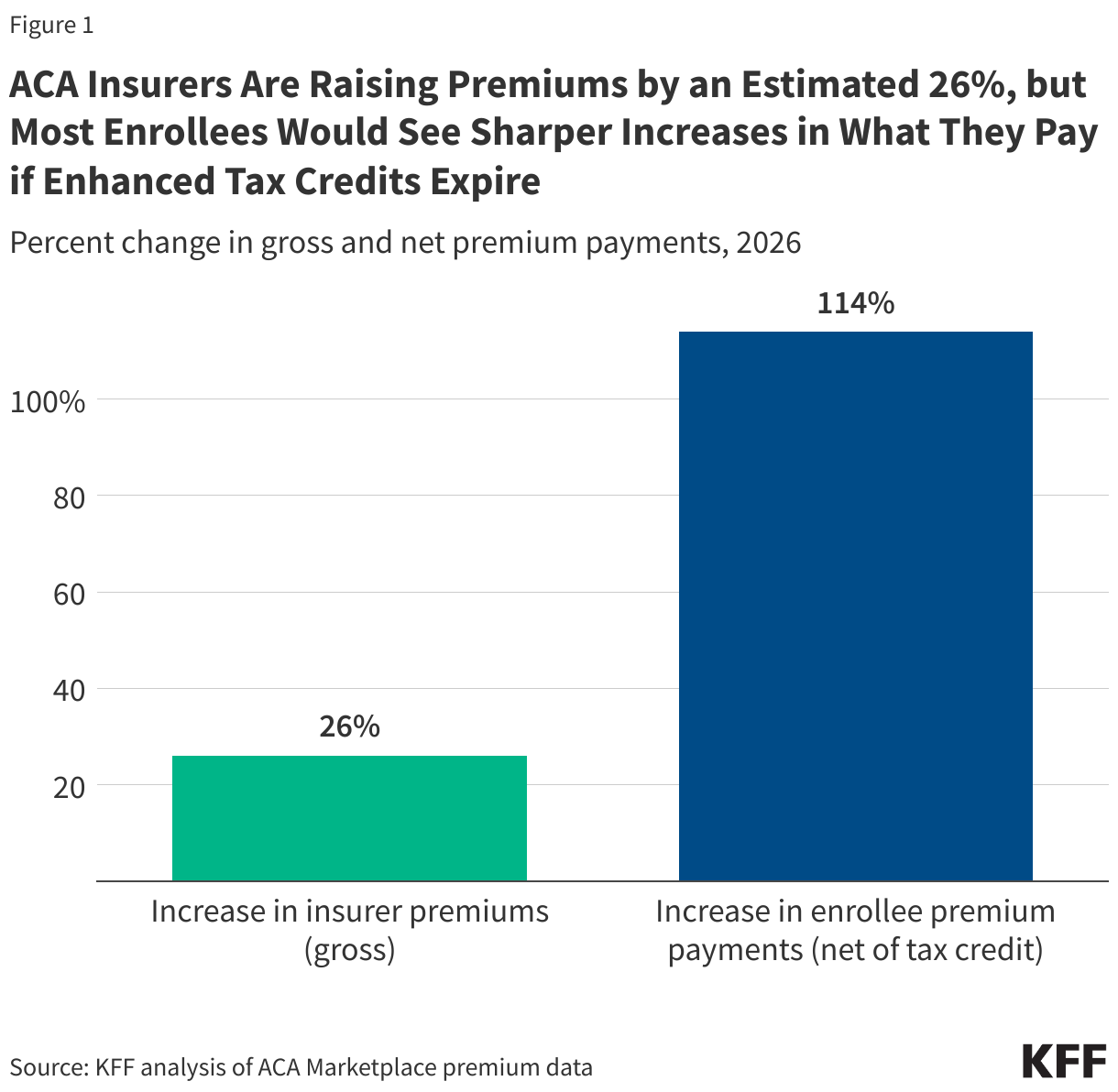
For the 93% of Marketplace (exchange) enrollees who are receiving premium subsidies (premium tax credits) for 2025 coverage, the after-subsidy premium for the benchmark (second-lowest-cost Silver) plan is projected to increase by 114% in 2026, unless Congress takes action to extend the subsidy enhancements that are scheduled to expire at the end of 2025.
For the 7% of Marketplace enrollees who don’t get subsidies – plus anyone who buys ACA-compliant individual market coverage outside the exchange – full-price (unsubsidized) premiums are increasing by an average of 26%, although this will vary considerably from one policy to another.
There are more than 23 million people with Marketplace coverage, and given the average rate increases, most of them could be experiencing some degree of sticker shock when they look at their 2026 premiums.
Here are five steps you can take to better understand changes in Marketplace insurance costs and take action during open enrollment.
1. Review the available plans. (Those won’t change.)
Insurers have finalized and received regulatory approval for the individual-market plans that are available in each state’s Marketplace for 2026. So although after-subsidy premiums could change if Congress takes action to extend or modify the subsidy enhancements, the coverage details of the available plans will not change.
That means you can take some time now to review details like deductibles, out-of-pocket maximums, covered drug lists, and provider networks, to get an idea of what your coverage options are for 2026. Your current plan might not be available for 2026, or there might be new plans available in your area, depending on where you live. And even in areas where plans continue to be offered by the same insurers that offered them in 2025, there could be changes in the coverage specifics.
2. Understand your income as a percentage of the federal poverty level (FPL)
Your eligibility for 2026 Marketplace premium subsidies is based on how your projected 2026 household income compares to the 2025 federal poverty level. (Note that these numbers are higher in Alaska and Hawaii.)
Here’s how household income (MAGI) is calculated under the ACA.
Unless Congress extends the subsidy enhancements, enrollees will no longer be eligible for premium subsidies in 2026 if their 2026 household income is more than 400% of the 2025 FPL. If you’re in the continental United States, here’s what 400% of FPL amounts to in annual income, for 2026 coverage:
- Household of one: $62,600
- Household of two: $84,600
- Household of three: $106,600
- Household of four: $128,600
- Household of five: $150,600
- Household of six: $172,600
This is why – unless Congress extends the subsidy enhancements – you’ll see no subsidy at all in the Marketplace if your projected household income is above those amounts. (If you’re in Massachusetts, New Jersey, or New Mexico, you may still see some subsidies, as those states have state-funded subsidies that extend to enrollees with incomes above 400% of FPL.)
3. Understand how HSA contributions can affect your MAGI
Consider a 60-year-old living in Atlanta, earning $63,000. (Here’s how ACA-specific modified adjusted gross income, or MAGI, is calculated.) At that income level, they’re just a little above 400% of FPL, which means they won’t qualify for any subsidy at all in 2026 if Congress doesn’t extend the subsidy enhancements. In that case, the lowest-cost plan available to this person will cost $1,079/month in premiums in 2026, which amounts to more than 20% of their household income.
But that lowest-cost option is a Bronze plan, and all Bronze Marketplace plans will allow enrollees to contribute to a health savings account (HSA) in 2026. So if this person enrolls in that Bronze plan, opens an HSA, and contributes just $1,000 to the HSA in 2026, that would bring their household income down to $62,000, which is just a little under 400% of FPL.
That would allow them to avoid the “subsidy cliff,” and would make them eligible for a significant subsidy. Their after-subsidy premium for that lowest-cost plan will drop to just $262/month – simply because they enrolled in an HSA-eligible plan, opted to contribute $1,000 to an HSA, and thus reduced their MAGI by $1,000.
That $1,000 HSA contribution (which is still their own money, and available at any time to pay for medical expenses on a pre-tax basis) results in them qualifying for a subsidy of $817/month, which covers the majority of the cost of their coverage.
This is just one example, and the specifics will vary depending on where you live, how old you are, how much you earn, and how much you’re able to contribute to an HSA. The maximum allowable HSA contribution for 2026 is $4,400 if you have self-only coverage, and $8,750 if your HSA-eligible health plan also covers at least one additional family member.
We recommend that you speak with a tax advisor if you’re considering this strategy, as there are tax ramifications when you make adjustments to your income. You should be aware of all of them before making any financial decisions.
4. Update your Marketplace account
Now is a good time to make sure your Marketplace account is up to date. If there have been any changes in your household or your income since the last time you updated your Marketplace account, be sure to report those changes to the Marketplace.
It’s particularly important to project your income as accurately as possible for 2026, and keep the Marketplace updated if you realize mid-year that your income projection wasn’t correct. This is because 2026 will be the first year when there’s no cap on how much excess advance premium tax credit (APTC) has to be repaid to the IRS.
If you underestimate your income and then end up earning more than you projected, there will be no limit on how much excess APTC you have to repay to the IRS when you file your taxes in early 2027.
5. Remember the Dec. 15 deadline (in most states) and stay tuned for updates
You have until at least December 15 (or later in some states) to pick a Marketplace plan that will take effect on January 1, 2026. So if you’re experiencing sticker shock when you see the prices that are currently displayed for 2026 coverage, you have a couple of options:
You can select a plan now, based on the prices that reflect the expiration of the subsidy enhancements.
If you do this, stay tuned for updates about the subsidy enhancements. If Congress later extends the subsidy enhancements or extends a modified version of them during open enrollment, you’ll have the option to pick a different plan if that’s your preference. The last plan you pick will take effect January 1, as long as you make the plan selection by December 15 (or the deadline in your state).
You can hold off on picking a plan for now, and stay tuned for updates regarding the federal subsidy enhancements.
If you decide to delay enrollment in the hopes that the subsidy enhancements will be extended by Congress, be sure to set a calendar reminder to enroll in a plan before December 15. If you don’t, your current Marketplace coverage will be auto-renewed. (If you’re currently uninsured, you’ll continue to be uninsured in January.) But actively selecting your own plan is generally a better option than relying on auto-renewal.
Louise Norris is an individual health insurance broker who has been writing about health insurance and health reform since 2006. She has written hundreds of opinions and educational pieces about the Affordable Care Act for healthinsurance.org.