Artificial intelligence (AI) is changing the way that people look for information – offering the promise of speedy searches and increasingly personalized answers. But if you’re hoping AI can be a personal shopper for health insurance that perfectly fits your healthcare needs and your budget, you should consider that AI can get a lot wrong.
How can AI help if you’re curious about health insurance?
As a health policy analyst, I’m aware that artificial intelligence is becoming a starting point for people who have questions about health insurance. And it makes sense: AI can sift through enormous amounts of historical information to explain concepts like the health insurance Marketplace, Medicaid, premium subsidies and cost-sharing reductions, and other forms of federal and state financial assistance. It can explain how deductibles and copays work, what the essential health benefits are, and how plans are categorized by metal level.
AI can also help consumers better understand the basics of how health coverage works. But after decades as both a health insurance broker helping consumers enroll in coverage and a health policy analyst tracking changes in federal and state rules, I’ve also seen where AI reaches its limits.
To test AI’s capabilities – and limitations – I did some basic searches that might be conducted by individual health insurance shoppers. In doing so, I identified some key challenges AI faces when answering your questions about health insurance:
1. Keeping up with constantly changing rules
Health insurance rules don’t just change every few years. Numerous provisions change each year, including premiums, plan designs, out-of-pocket limits, plan availability, the federal poverty level, and the percentage of income that a subsidy-eligible person has to pay for the benchmark plan.
Rules also evolve over time. Examples are changes to subsidy eligibility for immigrants starting in 2026 and 2027, the expiration of federal subsidy enhancements at the end of 2025, and the expansion of HSA-eligible plans to include all Bronze and Catastrophic Marketplace plans starting in 2026.
Example: When I asked Google, “Am I eligible for a health insurance subsidy?” its AI asked me to provide my household size and estimated household income, and my hypothetical response was a household of four with a $100,000 annual income.
The AI model told me that I qualify for a subsidy because a household of four is subsidy-eligible with an income up to $132,000. But that’s not the correct subsidy eligibility limit this year.
Subsidy eligibility extends to 400% of the federal poverty level (FPL) now that the “subsidy cliff” has returned, but it’s 400% of the prior year’s FPL, not the current year’s FPL.
So for 2026 coverage, subsidy eligibility in the continental U.S. ends at $128,600, which is 400% of the 2025 FPL. The AI model was using 400% of the 2026 FPL, which won’t be used to determine subsidy eligibility until the 2027 plan year.
Another example? When I prompted Google to calculate the actual subsidy amount, it replied, “Under standard ACA rules, households making between 300% and 400% of the FPL are expected to contribute up to 9.5% of their annual household income toward a benchmark health plan.”
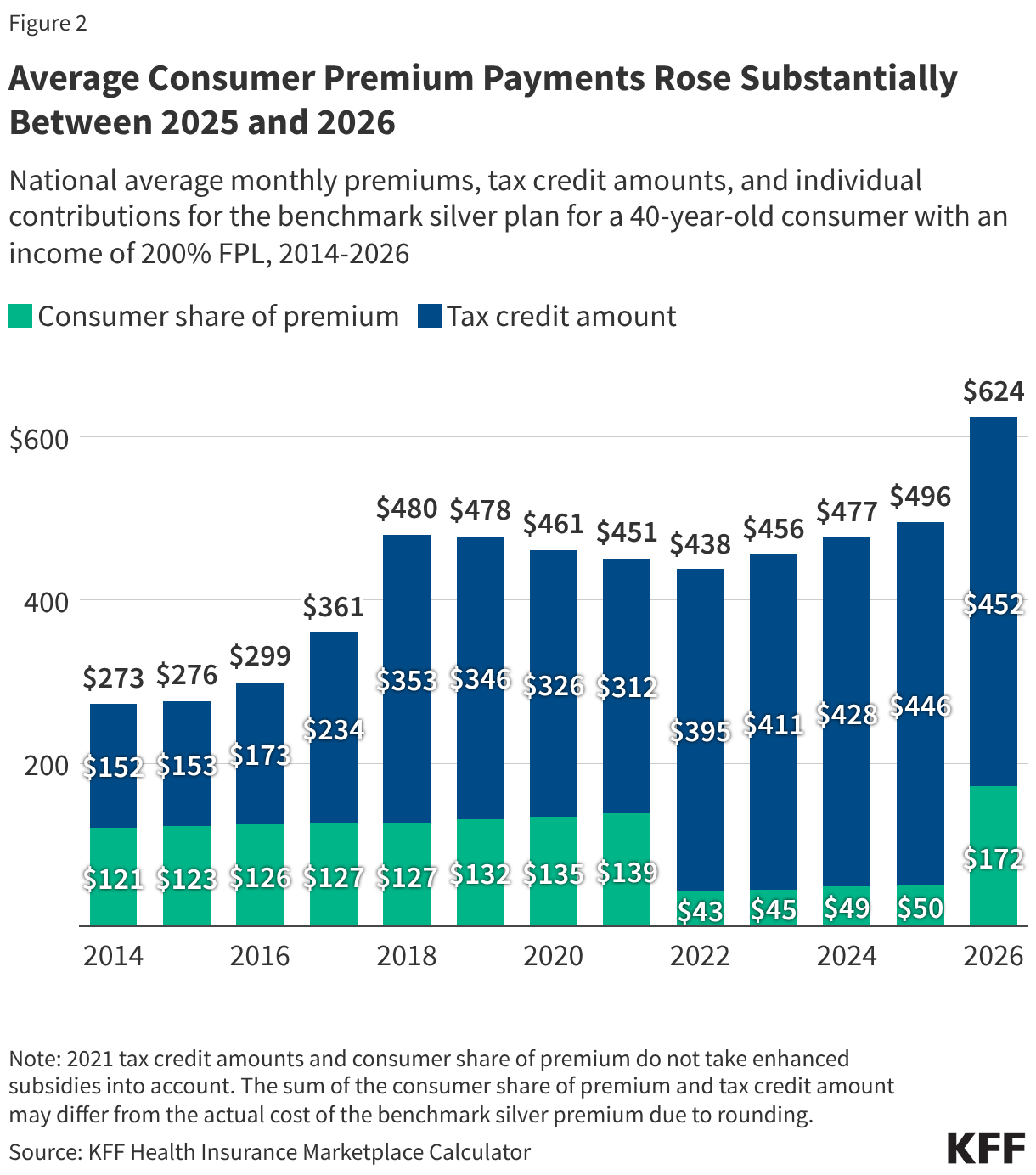
What the AI model failed to understand is that while the expected contribution percentage started at 9.5% under the ACA in 2014, it is indexed annually by the IRS. In 2026, a household with income between 300% and 400% of the prior year’s FPL is expected to pay 9.96% of household income toward the benchmark plan (the second-lowest-cost Silver plan).
So when the AI model continued the calculation using 9.5% rather than 9.96%, it ended up understating how much the household would have to pay, and overstating how much the subsidy would be.
2. Understanding how different programs interact
Health coverage in the U.S. is made up of a patchwork of multiple types of coverage. Depending on a person’s circumstances, they might qualify for Marketplace subsidies (including state-funded subsidies in some states), full-price Marketplace coverage, Medicaid, a Basic Health Program, the Children’s Health Insurance Program (CHIP), Medicare, or employer-sponsored coverage.
So before we can determine whether a person is eligible for Marketplace subsidies, we have to first ensure that they aren’t eligible for any other coverage programs, such as Medicaid or an employer’s group plan. And an AI model won’t always get that correct.
For example, when I told Google’s AI that I’m a single Colorado resident earning $21,000, it concluded that I was “highly likely” to qualify for a subsidy, and that I would also qualify for Colorado’s state-funded subsidy of $80/month.
But neither of those is true. In Colorado (as is the case in DC and 39 other states), a person earning $21,000 this year is not eligible for subsidies, because they’re eligible for Medicaid instead. (Under the ACA, expanded Medicaid is available to adults with household income up to 138% of the current year’s FPL; in the continental U.S. in 2026, that’s $22,024 for a single person.)
3. Making assumptions based on conventional wisdom
Choosing health insurance isn’t simply about picking the plan with the lowest deductible or the richest benefits. Health insurance decisions often require comparing premiums, deductibles, out-of-pocket maximums, provider networks, prescription coverage, tax advantages such as HSAs, and expected utilization simultaneously. That’s a far more complex analysis than applying a general rule of thumb.
Example: In a conversation with ChatGPT, I said that I am 50 years old, live in Dallas, earn $80,000 per year, need double hip replacement surgery (each of which costs an average of about $39,000, meaning the maximum out-of-pocket limit will be reached on any ACA-compliant policy), and wanted help picking a Marketplace plan. I said that I hadn’t chosen a surgeon yet, so I was willing to consider any in-network providers for any of the available policies.
ChatGPT correctly noted that with an income of $80,000, I wouldn’t be eligible for Marketplace subsidies. But it also told me that “Bronze plans are usually a poor choice if you already know a major surgery is coming, because you’ll likely end up paying much of the deductible and cost-sharing anyway.” That’s in line with conventional wisdom, as people often believe that a plan with lower out-of-pocket costs is the better option if you know you’re going to need a lot of care. But you also have to add premiums into the equation.
I used HealthCare.gov’s plan comparison tool to get unsubsidized 2026 quotes for a 50-year-old in Dallas. Here are the total costs for a full year of premiums plus maximum out-of-pocket expenses for the lowest-premium Marketplace plan at each level:
- Catastrophic: $17,501 ($6,901 in premiums plus $10,600 in out-of-pocket costs)
- Bronze: $17,864 ($7,264 in premiums plus $10,600 in out-of-pocket costs)
- Silver: $20,093 ($11,193 in premiums plus $8,900 in out-of-pocket costs)
- Gold: $18,866 ($9,866 in premiums plus $9,000 in out-of-pocket costs)
(Note: The cost illustration includes premiums for the full year, assuming this person enrolled during the open enrollment period. If you sign up later in the year using a special enrollment period, your premiums would be prorated for the number of months you have coverage, but the out-of-pocket maximum would not change.)
In this case, if the person is happy with the in-network surgeons and facilities in the lowest-cost Catastrophic plan’s network, that plan will result in the lowest total costs. It has a maximum out-of-pocket limit of $10,600, which is higher than the out-of-pocket limits for the Silver and Gold plans. But the lower premiums more than offset the higher out-of-pocket costs.
It’s also important to note that all Catastrophic and Bronze Marketplace plans are now HSA-eligible. So if this person selects a Catastrophic or Bronze plan, they’ll be able to put up to $4,400 into a health savings account in 2026. That contribution will be pre-tax, and they’ll be able to withdraw it (still tax-free) to pay some of their out-of-pocket costs.
This example highlights why it’s not a great idea to make assumptions based on conventional wisdom when picking a health plan, which the AI model was doing.
4. Accounting for differences in state insurance programs
Some states have expanded Medicaid. Others have not. Some operate Basic Health Programs. Others offer state-funded subsidies or have unique enrollment rules.
So an answer about program eligibility that’s correct in Texas may be completely wrong in Colorado or Minnesota.
Example: I started by simply asking ChatGPT what Marketplace health policy I should choose. When it asked me where I live, how much I earn, and how much health care I think I might need, I told it that I live in Minnesota and earn $30,000. That would make me eligible for Minnesota’s Basic Health Program (BHP), MinnesotaCare. So the correct response would be to tell me that, and then provide guidance on choosing a managed care organization to provide my MinnesotaCare coverage.
But instead, ChatGPT incorrectly told me that I’d be eligible for premium subsidies and cost-sharing reductions via MNsure (the state-run Marketplace in Minnesota). To clarify, if a person is eligible for BHP coverage, they are not eligible for Marketplace subsidies.
5. Accounting for state-specific health insurance rules
Other examples of state-specific differences that could trip up AI?
- Alaska and Hawaii have different FPLs than the other 48 contiguous states and D.C., so the income level that makes a person subsidy-eligible is different in those states.
- Washington, D.C., Minnesota, New York, and Oregon have Basic Health Programs for people who earn too much for Medicaid but not more than 200% of FPL. So subsidy eligibility starts above 200% of FPL in those states.
- Ten states provide state-funded subsidies to some Marketplace enrollees (including enrollees with income above 400% of FPL in New Jersey and New Mexico).
- Carrier participation in the Marketplace varies considerably from one state to another, and sometimes changes from one year to the next (see details about carrier exits and entries for 2027).
- Within a given state, Marketplace carriers often have different service areas. This is why accurate health insurance quotes always require a zip code.
- American Indians and Alaska Natives get benefits and enrollment opportunities that aren’t available to other applicants.
Back up any AI research by checking reliable sources
An AI model may help you identify questions to ask and details that might apply to your specific circumstances. But keep in mind that AI answers can sound convincing, even when they’re incorrect.
Augment AI research, using official sources to verify the information you get from the AI tool. Seek out an agent in your area who can help you understand all the nuances and pick a plan.
A local broker or Navigator will provide you with zero-cost assistance. They’ll be familiar with all of the plans available in your area, and have a good understanding of each plan’s provider network. They’ll know about specific details like access to Medicaid or a BHP, how rates and plans are changing for the coming year, and whether there are any state-specific subsidies available. They’ll also be able to explain how subsidies get reconciled on your tax return.
Got questions? Healthinsurance.org has resources that can help: